
Expanding Midwifery Scope & The Midwifery Model
“Abortion care deserves the same tenderness we provide to people that carry pregnancies to term”
-Anonymous

“Expanding the scope of practice for midwives will support healthy pregnancies and improve access to essential, culturally safe reproductive care for people in communities where it might be limited.”
As of April 1, Midwives with the appropriate certification will be able to prescribe and manage early miscarriage or medical abortion within the first trimester using Mifegymiso. Click on the photo to review the news link for this update. Stay tuned for more information from the BCCNM and MABC to learn how to certify this skill and integrate it into your practice.
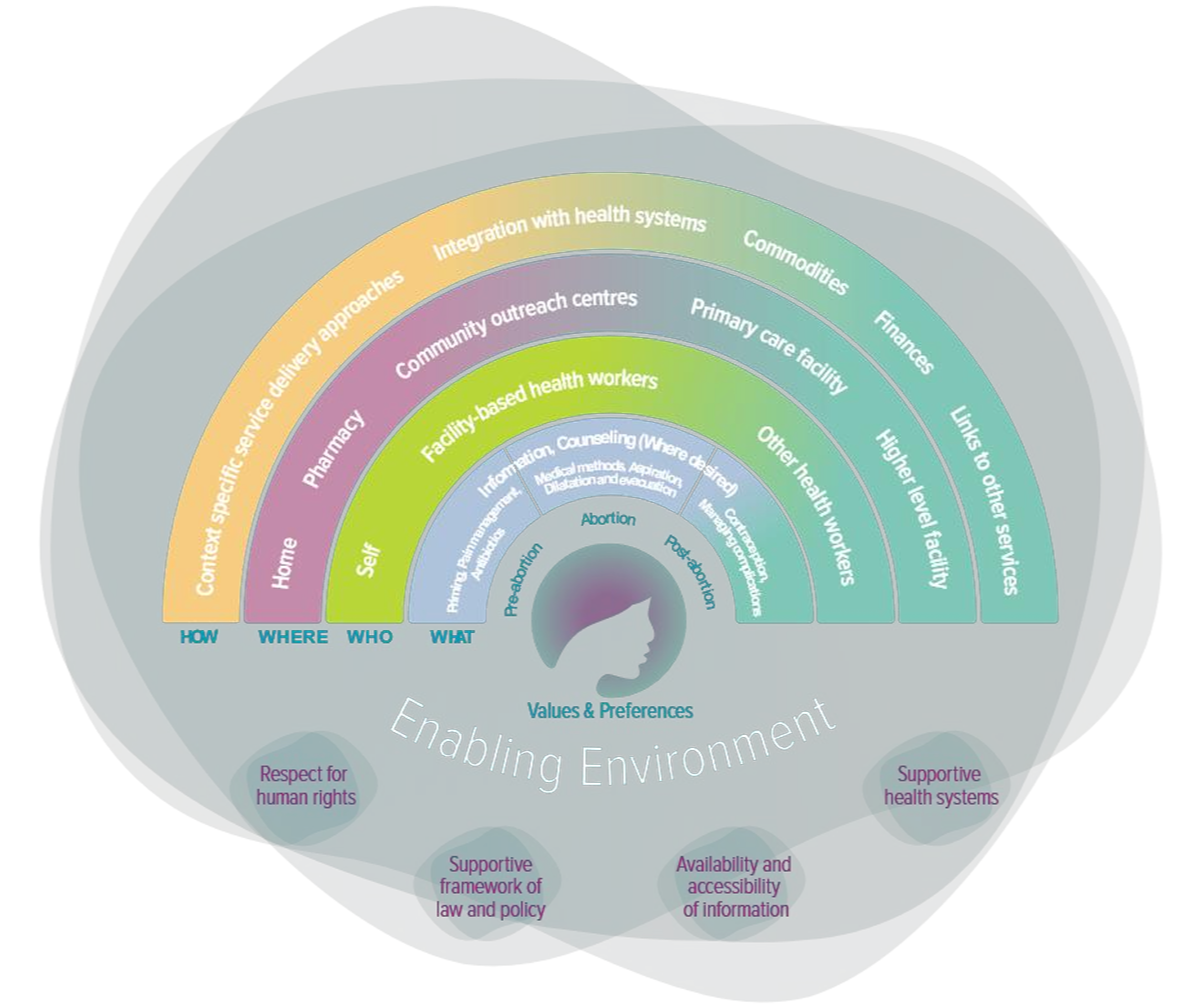
why are midwives well-positioned to provide abortion care?
Community-Based Primary Care
Abortion is a normal part of reproductive health care, and reproductive health care is central to midwifery care (CAM)
The midwifery scope of practice includes the management of all forms of abortion, including spontaneous (miscarriage), therapeutic, incomplete, and missed (CAM)
Access to early abortion makes abortion safer for clients and more cost-effective for the healthcare system (CAM)
This is especially important in rural locations so people can access timely care at home
Continuity of Care
Abortion provision is part of continuity of care; many people seeking abortion have previously given birth, and for midwifery clients, returning to their midwife for abortion care may be preferable to other options (CAM)
Informed Choice
Abortion includes planned and unplanned pregnancies (CAM)
The midwifery model of care is ideally suited to support access to all forms of abortion care (CAM)
Choice of Birth Place
Midwives can support clients to have a medication abortion in the safety and comfort of their own home
This is particularly important for some people in terms of cultural safety and rites
Collaborative Care
Midwives frequently work with interprofessional colleagues to increase and ensure access to abortion care in their communities (CAM)
Expanding qualified abortion providers to include midwives will increase access to medical abortion and thus reduce the number of procedural abortions (CAM)
World Health Organization (WHO). (2022, March 23) Abortion care guideline: Resource kit.
What skills do midwives have that are applicable to abortion care provision?
Trauma-informed, culturally inclusive model of care
Indigenous midwives have long had the knowledge and the means to provide abortion care, responsive to the local needs, context, and practices of their communities (CAM)
Training and experience in managing pregnancy loss, stillbirth, and pre- and post-abortion care
Well positioned to provide medication abortion due in large part to RMs’ existing skill sets (e.g. assessment and triage skills; management of postpartum hemorrhage, which requires an understanding of the pharmacokinetics of misoprostol) (Dowler, Rushton, & Kornelsen, 2019)
Specialized Practice Certification in Contraceptive Prescribing allows RMs to provide a continuum of care for patients seeking medication abortion, including counseling on contraceptive options where appropriate (Dowler, Rushton, & Kornelsen, 2019)
Increasing Access to Abortion Care (UBC CPD)
All healthcare providers have a role to play in abortion care, though they may not directly prescribe or perform terminations. Anyone can be the first point-of-contact, and your actions and reactions have the potential to influence how a pregnant person feels about their options. Here are some examples of supportive and open-ended language to use when discussing abortion:
“How do you feel about being pregnant right now?”
“I know that faith and religion play a different role for every person. How is yours impacting your decision about contraception and conception?”
“I don’t know the answer - let’s look into it together”
“How would your life be different in 12 months (or 12 years) if you continue this pregnancy?”
Key Discussion Strategies:
Exercise empathy
Match client’s language and tone
Educate and dispel rumours/misconceptions (advocate)
Consider translation options where applicable
Your Role
-
Keep an eye out for training from the BCCNM and MABC and stay updated on culturally relevant practices in your local context.
Engage with your community to find out what resources already exist and where mentorship may be available to you.
Consider becoming a member of Abortion Care Canada.
Keep cultural safety and personal safety at the forefront of your evolving practice. Check in with the Fireweed Project, NCIM, and the MABC as needed.
Check in with yourself about your personal beliefs and how they impact your conversations about choice.
Be aware of Anti-Choice Movements and Organizations. A comprehensive list of such organizations can be found here: https://www.antichoice.ca/
We strongly recommend you check out the resources linked below.
-
Keep an eye out for training from the BCCNM and MABC and stay updated on culturally relevant practices in your local context.
Engage with your community to find out what resources already exist and how to refer appropriately. Check out the BCCNM guideline on Conscientious Objection and the Duty to Provide Care (for Nurses) and stay tuned for a document pertaining to midwives.
Consider becoming a member of Abortion Care Canada.
Keep cultural safety and personal safety at the forefront of your evolving practice. Check in with the Fireweed Project, NCIM, and the MABC as needed.
Check in with yourself about your personal beliefs and how they impact your conversations about choice.
Be aware of Anti-Choice Movements and Organizations. A comprehensive list of such organizations can be found here: https://www.antichoice.ca/
We strongly recommend you check out the resources linked below.
-
Engage with your community to find out what resources already exist and how to refer appropriately.
Review how to discuss abortion with clients and know how to speak about it in a trauma-informed and unbiased way. Engage with your community to find out what resources already exist and how to refer appropriately. Check out the BCCNM guideline on Conscientious Objection and the Duty to Provide Care (for Nurses) and stay tuned for a document pertaining to midwives.
Check in with yourself about your personal beliefs and how they impact your conversations about choice.
Be aware of Anti-Choice Movements and Organizations. A comprehensive list of such organizations can be found here: https://www.antichoice.ca/
We strongly recommend you check out the resources linked below.
-
Talk to your colleagues who are prescribers and find mentorship in the community. Start by reading this website to learn more about abortion in Canada and in BC!
Keep an eye out for training from the BCCNM and MABC and stay updated on culturally relevant practices in your local context.
Check in with yourself about your personal beliefs and how they impact your conversations about choice.
Be aware of anti-choice movements and organizations. A comprehensive list of such organizations can be found here: https://www.antichoice.ca/.
We strongly recommend you check out the resources linked below.
Cultivating a Respectful Workplace for abortion care providers and conscientious objectors
Proactive conversations are recommended, rather than reactive; approach with curiosity, not ferocity
Best to include unbiased and evidence-based information
Know about conscientious objection and your duty to refer within a reasonable timeline
Regardless of personal beliefs, healthcare providers are not permitted to actively block or dissuade a pregnant person from accessing an abortion; we all have a responsibility to provide accurate, timely, and unbiased care.
Canadian Medical Association: Code of Ethics and Professionalism
“...ethical practice is understood as a process of active inquiry, reflection, and decision-making concerning what a [provider]’s actions should be and the reasons for these actions. The code informs ethical decision-making, especially in situations where… values and principles are in tension”
In the context of the patient-physician relationship, points 3-5:
“Act according to your conscience and respect differences of conscience among your colleagues; however, meet your duty of non-abandonment to the patient by always acknowledging and responding to the patient’s medical concerns and requests whatever your moral commitments may be
Inform the patient when your moral commitments may influence your recommendation concerning provision of, or practice of any medical procedure or intervention as it pertains to the patient’s needs or requests.
Communicate information accurately and honestly with the patient in a manner that the patient understands and can apply, and confirm the patient’s understanding”
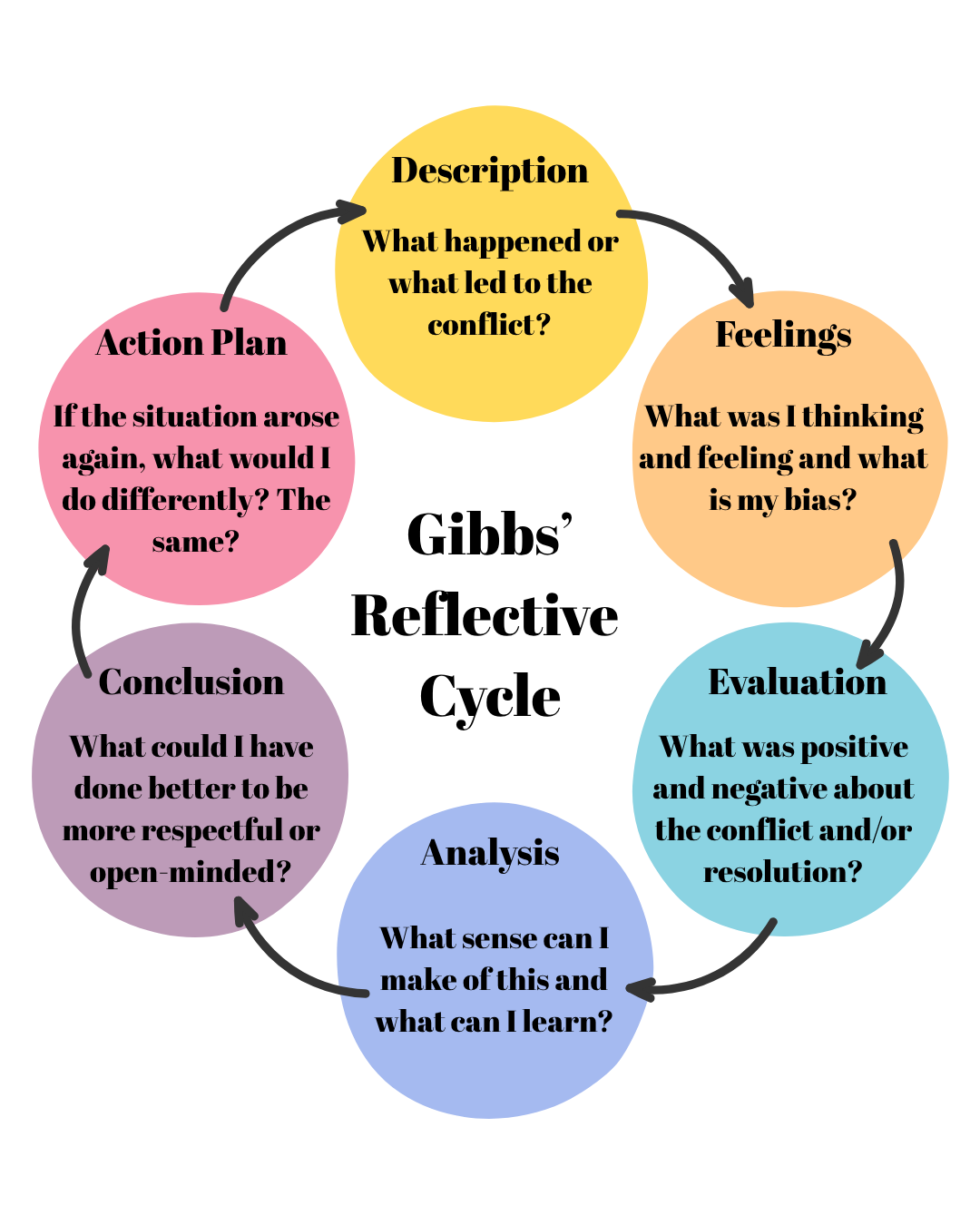
Reflection
How do your biases impact how you provide care in varying aspects of midwifery? How do you check in with these feelings?
How do you usually hold compassion for people with different opinions from you?
What can you do to provide safe care to people, regardless of whether or not you choose to prescribe Mifegymiso?
How will you keep yourself safe as an abortion care provider? Will you advertise that you provide these services?